
Antifungal Selection Tool for Candidemia
Clinical Guidance
Based on IDSA 2023 guidelines for candidemia treatment. Select options below to receive appropriate therapy recommendations.
Hospital wards are wrestling with a silent enemy that’s slipping past traditional defenses: candidemia is a bloodstream infection caused by Candida species, and when the fungus spreads beyond the blood to organs such as the eyes, brain, or kidneys, it becomes a disseminated candida infection. Both conditions carry steep mortality rates, and recent data show they’re climbing faster than many clinicians anticipate. This article breaks down why the threat is growing, who’s most vulnerable, how to catch it early, and what frontline teams can do to keep patients safe.
What Exactly Is Candidemia?
In plain terms, candidemia is the presence of Candida yeast in the bloodstream. While yeast normally lives harmlessly on skin and mucous membranes, it can enter the circulatory system through breaches such as IV catheters, surgical wounds, or a compromised gut barrier. Once in the blood, the organism can hitch a ride to distant organs, turning a relatively simple infection into a full‑blown systemic crisis.
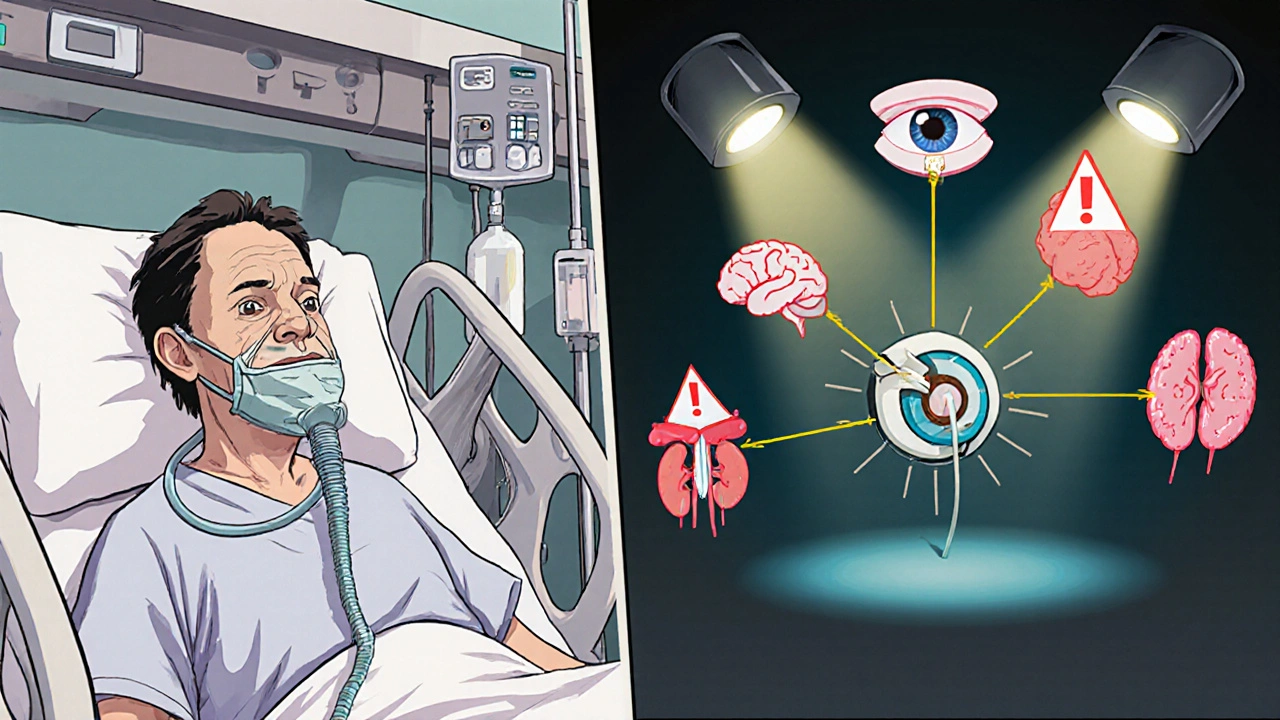
Understanding Disseminated Candida Infections
When Candida moves beyond the bloodstream, it can seed multiple organs-a condition clinicians label disseminated candida infection. Typical sites include the eye (endophthalmitis), brain (meningoencephalitis), heart (endocarditis), and kidneys. The clinical picture is often vague-fever, low blood pressure, or organ‑specific dysfunction-making diagnosis a race against time.
Who’s Most at Risk?
- Intensive Care Unit (ICU) patients: Prolonged ventilation, central venous catheters, and frequent antibiotic use create a perfect storm.
- Those with neutropenia from chemotherapy or bone‑marrow transplants.
- Patients undergoing major abdominal surgery or with severe gastrointestinal perforation.
- Individuals with total parenteral nutrition (TPN) administered through central lines.
- People colonized with resistant species such as Candida auris.
Why Are Cases on the Rise?
Three interlocking trends are driving the surge:
- Increasing use of invasive devices. More patients receive central lines, urinary catheters, and ECMO support, each offering a portal for yeast.
- Broad‑spectrum antibiotic pressure. When bacterial flora are wiped out, Candida faces less competition and can proliferate unchecked.
- Emerging antifungal resistance. Species like Candida auris and fluconazole‑resistant Candida glabrata are spreading worldwide, limiting the effectiveness of first‑line drugs.
Data from the CDC’s 2024 Antimicrobial Resistance Surveillance Program show a 12% annual increase in hospital‑onset candidemia, with mortality climbing from 38% to 45% over the past five years.
How Do We Diagnose It?
Early detection hinges on a combination of clinical suspicion and rapid laboratory tools.
- Blood cultures. Still the gold standard but can take 48‑72 hours to turn positive.
- Beta‑D‑Glucan assay. Detects fungal cell wall components in serum; a negative result helps rule out invasive candidiasis.
- T2Candida Panel. A PCR‑based test that delivers species‑level identification in 3‑5 hours, dramatically trimming the time to appropriate therapy.
- Imaging. CT or MRI can reveal organ involvement when disseminated infection is suspected, especially for liver, spleen, or brain lesions.
When a patient meets high‑risk criteria (e.g., ICU stay > 7 days, central line in place, broad‑spectrum antibiotics), many institutions now start empiric antifungal therapy while waiting for culture confirmation.
First‑Line Treatment Options
The IDSA 2023 guidelines recommend echinocandins (caspofungin, micafungin, anidulafung) as the preferred initial agents for most adult patients because of their broad spectrum and low resistance rates.
| Class | Representative Drugs | Mechanism | Typical Use | Notable Side Effects |
|---|---|---|---|---|
| Echinocandins | Caspofungin, Micafungin, Anidulafung | Inhibit β‑1,3‑glucan synthesis | First‑line for most adults | Elevated liver enzymes, infusion reactions |
| Azoles | Fluconazole, Voriconazole, Itraconazole | Inhibit ergosterol synthesis (lanosterol 14α‑demethylase) | Step‑down after stabilization; specific species (C. albicans) susceptible | Hepatotoxicity, QT prolongation, drug‑drug interactions |
| Polyenes | Amphotericin B (deoxycholate, lipid formulations) | Bind ergosterol, create membrane pores | Rescue therapy for resistant strains | Nephrotoxicity, infusion fever |
If a Candida species shows resistance to echinocandins (rare but reported in C. auris), high‑dose fluconazole or lipid‑formulation amphotericin B become alternatives. Therapeutic drug monitoring is essential for azoles to avoid toxicity.
Preventing Hospital‑Acquired Candidemia
Prevention is a team sport. Hospitals that have cut candidemia rates by half rely on a bundle of interventions:
- Catheter hygiene protocols. Daily review of line necessity, antimicrobial‑impregnated catheters, and chlorhexidine skin prep.
- Antifungal stewardship. Restrict empiric azole use, enforce de‑escalation based on culture data.
- Environmental cleaning. UV‑C disinfection and dedicated equipment for rooms housing C. auris patients.
- Rapid diagnostics. Implementing T2Candida or MALDI‑TOF on positive cultures shortens time to targeted therapy.
- Nutrition management. Minimize TPN duration and use peripheral lines when possible.
Education of bedside nurses and physicians about early signs-persistent fever despite antibiotics, new organ dysfunction-also raises the index of suspicion.
Emerging Threat: Candida auris
First identified in 2009, C. auris is now a global concern. It thrives on hospital surfaces, resists many disinfectants, and shows multi‑drug resistance (often to fluconazole, amphotericin B, and sometimes echinocandins). Outbreaks in UK intensive care units have prompted the NHS to issue specific infection‑control guidance, including mandatory screening of contacts and cohort isolation.
Rapid identification using MALDI‑TOF or whole‑genome sequencing is critical; misidentification as C. parapsilosis can lead to ineffective therapy.
Key Takeaways Checklist
- High‑risk patients: ICU, central lines, neutropenia, TPN.
- Watch for persistent fever > 48 h despite broad‑spectrum antibiotics.
- Order blood cultures plus beta‑D‑glucan or T2Candida for faster results.
- Start echinocandin empirically; switch to azole only after susceptibility confirmed.
- Implement catheter‑care bundles and antifungal stewardship to curb incidence.
- Be vigilant for C. auris; isolate promptly and clean environment thoroughly.
Frequently Asked Questions
What is the difference between candidemia and a Candida bloodstream infection?
Both terms describe Candida in the blood. “Candidemia” is the clinical diagnosis; “Candida bloodstream infection” is a broader phrase that includes the same condition. In practice they are used interchangeably.
How long does it take for blood cultures to grow Candida?
Standard aerobic bottles usually become positive within 48‑72 hours, but some slow‑growing species may need up to 5 days.
Can candidemia be prevented without removing central lines?
Complete avoidance is rare, but stringent insertion techniques, chlorhexidine dressings, and daily necessity checks can dramatically lower risk while keeping the line in place when it’s essential.
When should I switch from an echinocandin to fluconazole?
After blood cultures identify a fluconazole‑susceptible species (e.g., C. albicans) and the patient is clinically stable, a step‑down to oral fluconazole is recommended, typically after 5‑7 days of IV therapy.
Is Candida auris more deadly than other Candida species?
Mortality rates for C. auris range from 30‑60 % depending on the outbreak and treatment delays, which is comparable or slightly higher than traditional species due to resistance and delayed appropriate therapy.
What role does antifungal stewardship play in controlling candidemia?
Stewardship programs audit antifungal prescriptions, ensure drugs are used only when indicated, and promote early de‑escalation. Hospitals with active stewardship have reported up to a 40 % reduction in candidemia incidence.

Ian Glover
My name is Maxwell Harrington and I am an expert in pharmaceuticals. I have dedicated my life to researching and understanding medications and their impact on various diseases. I am passionate about sharing my knowledge with others, which is why I enjoy writing about medications, diseases, and supplements to help educate and inform the public. My work has been published in various medical journals and blogs, and I'm always looking for new opportunities to share my expertise. In addition to writing, I also enjoy speaking at conferences and events to help further the understanding of pharmaceuticals in the medical field.
9 Comments
-
Christopher Burczyk
October 21, 2025 AT 03:26Early identification of candidemia remains paramount; beta‑D‑glucan assays and the T2Candida panel dramatically reduce time to appropriate therapy.
Blood cultures, while still gold standard, should be obtained promptly, acknowledging the inherent 48‑72‑hour delay.
Empiric echinocandin use in high‑risk ICU patients aligns with IDSA recommendations and improves survival odds.
Institutions that integrate rapid diagnostics into stewardship protocols report measurable mortality reductions. -
dennis turcios
October 22, 2025 AT 10:00The article oversimplifies the resistance issue; ignoring regional variability does a disservice to clinicians.
A nuanced discussion of azole cross‑resistance would have been more appropriate. -
sravya rudraraju
October 23, 2025 AT 16:33The rise of candidemia in hospital settings cannot be attributed to a single factor, but rather a confluence of modern medical practices.
Invasive devices such as central venous catheters and ECMO circuits provide direct portals for yeast to enter the bloodstream.
Broad‑spectrum antibiotics, while lifesaving, eradicate bacterial competitors and create ecological niches that favor Candida overgrowth.
Moreover, the emergence of multidrug‑resistant species like Candida auris complicates therapeutic choices and demands vigilant infection control.
Early detection hinges on a high index of suspicion, especially among patients who have sustained fevers beyond 48 hours despite appropriate antibacterial coverage.
Rapid assays, including beta‑D‑glucan and the T2Candida molecular panel, should be ordered concurrently with blood cultures to shorten the diagnostic window.
Once candidemia is suspected, initiating an echinocandin promptly, as per IDSA guidelines, is essential to curb mortality.
De‑escalation to an azole is only reasonable after species identification and susceptibility testing confirm susceptibility.
Equally important is the removal or replacement of any potentially contaminated intravascular device as soon as clinically feasible.
Antifungal stewardship programs must track usage patterns, discourage indiscriminate azole prophylaxis, and enforce step‑down protocols.
Environmental decontamination, particularly in areas housing C. auris patients, should incorporate agents proven effective against fungal spores, such as chlorine‑based disinfectants or UV‑C light.
Nutrition teams can also contribute by limiting the duration of total parenteral nutrition and opting for peripheral routes whenever possible.
Education of frontline nurses and physicians about the subtle signs of disseminated infection, such as new organ dysfunction, further raises the index of suspicion.
Multidisciplinary rounds that include infectious disease specialists, pharmacists, and microbiologists foster coordinated decision‑making.
Data collection on candidemia incidence allows benchmarking against national trends and identification of local outbreaks.
Ultimately, a comprehensive bundle that integrates device hygiene, rapid diagnostics, stewardship, and education is the most effective strategy to reverse the upward trajectory of hospital‑acquired candidemia. -
Ben Bathgate
October 24, 2025 AT 23:06Good points, especially about swapping out catheters early; that alone can drop infection rates.
Keeping a daily line checklist is a simple win. -
Ankitpgujjar Poswal
October 26, 2025 AT 04:40Take charge of line maintenance, run daily audits, and never settle for ‘it’s just a line’-that’s how you win against Candida.
-
Bobby Marie
October 27, 2025 AT 11:13Candida auris needs a dedicated cleaning protocol.
-
Thokchom Imosana
October 28, 2025 AT 17:46Behind the push for rapid diagnostics lies a coordinated effort by pharma giants to steer hospitals toward high‑margin antifungals.
The data showing a 12% yearly rise is selectively reported to justify larger drug budgets.
Many institutions adopt new panels without questioning whether they truly change outcomes, but mainly to boost device sales.
It's no coincidence that the same manufacturers also market expensive echinocandins as first‑line therapy.
We should remain skeptical about the narrative that technology alone will solve the candidemia surge. -
ashanti barrett
October 30, 2025 AT 00:20We must champion real‑time antifungal stewardship and support staff with the tools they need, because every delayed dose costs a life.








Write a comment
More Articles
Flunarizine interactions with other medications: A guide for patients
Well, folks, let's dive into the exciting world of Flunarizine interactions! A medication often used for migraines and vertigo, Flunarizine is as social as a prom queen at a high school reunion, mixing and mingling with other drugs in your system. It's like a cocktail party, but in your body! Now, this party can turn into a bummer if mixed with alcohol or antihypertensives, potentially causing dizziness or even fainting. So, as always, it's important to chat with your doctor about all the medications you're taking, to ensure the party in your system stays fun and safe!

Clopidogrel, Prasugrel, and Ticagrelor: Side Effects Compared (2026 Guide)
Choosing the right antiplatelet drug is critical for heart patients. This guide compares the side effects of clopidogrel, prasugrel, and ticagrelor, including bleeding risks, dyspnea, and expert preferences. Updated for 2026.
Ampicillin and biofilms: Can it help break down bacterial communities?
In my latest research, I came across an interesting topic about Ampicillin and its potential role in breaking down bacterial communities known as biofilms. Biofilms are notorious for their resistance to antibiotics, making infections difficult to treat. Ampicillin, a widely used antibiotic, has shown some promise in disrupting these communities. Studies have suggested that it could weaken the biofilm structure, making it easier for other antibiotics to penetrate and eliminate the bacteria. It's fascinating to think that a common antibiotic like Ampicillin might be the key to tackling these stubborn bacterial communities!
Sarah Unrath
October 19, 2025 AT 20:53Candidemia is real and we need better line care