Medication Side Effect Risk Calculator
Enter your situation to see your side effect risk score. The calculator uses real-world data from the article to show how telehealth interventions reduce risk.
Your Risk Score
For millions of people living in rural and remote areas, taking medication for chronic conditions like high blood pressure, depression, or blood clots comes with a hidden risk: side effects. These reactions can be dangerous, even life-threatening. But getting to a doctor for a check-up? That might mean driving 70 miles over dirt roads, taking half a day off work, or waiting weeks for an appointment. In many cases, patients don’t report symptoms until it’s too late. That’s where telehealth comes in-not as a luxury, but as a lifeline.
Why Rural Patients Are at Higher Risk
Rural patients face a perfect storm when it comes to medication safety. According to the Health Affairs analysis from 2020, they experience 23% more preventable adverse drug events than people in cities. Why? It’s not just distance. Many rural clinics are understaffed. Pharmacists are scarce. Emergency care is hours away. And nearly 42% of people in frontier areas don’t have reliable broadband, making even simple video calls impossible. Worse, 36% of rural adults have low health literacy. They might not know what ‘dizziness’ or ‘bruising easily’ means in relation to their blood thinner. They might think fatigue is just aging. Or they might be too proud to admit they’re struggling. In urban settings, patients can walk into a pharmacy or clinic. In rural areas, silence often means danger.How Telehealth Monitoring Actually Works
Modern telehealth for side effect monitoring isn’t just a Zoom call. It’s a system. A network of tools working together to catch problems before they become emergencies. At the core are remote patient monitoring (RPM) devices. These include Bluetooth-enabled blood pressure cuffs, smart scales that track fluid weight, and wearable heart rate monitors. Devices like those from Yosi Health are FDA-cleared and accurate within ±3% for blood pressure and ±2 beats per minute for heart rate. Patients use them daily at home. Data syncs automatically to a secure platform. Then there’s the human side. Weekly video visits with a pharmacist or nurse. Patients report symptoms like nausea, tremors, or confusion. If a patient’s INR (a blood clotting measure) spikes on their monitor, the system alerts the care team immediately. In one program at the University of Mississippi, this caught dangerous bleeding risks before symptoms appeared-saving lives. Medication adherence is tracked too. Smart pill dispensers like Hero Health open only at scheduled times and log when doses are taken. If a patient misses a dose, the system sends a text reminder. If they miss two in a row, a nurse calls. Studies show this boosts adherence from 62% to 89%.What Works Best: Real-World Examples
Not all telehealth programs succeed. The difference? Structure. The University of Mississippi’s anticoagulation program uses three key pieces: a Bluetooth INR monitor, weekly pharmacist video visits, and a care coordinator who follows up with patients who miss appointments. Result? 92% of patients stay in the program for over a year. In Arkansas, a pilot program uses wearable sensors to detect subtle movement changes in patients taking antipsychotic drugs. These sensors pick up early signs of tardive dyskinesia-a side effect that can become permanent if not caught. The system detected issues with 91% accuracy in early tests. Even audio-only calls are making a difference. Since the 2023 CONNECT for Health Act, Medicare now covers phone check-ins for side effect monitoring. That’s huge for seniors who don’t have smartphones or reliable internet. In rural West Virginia, one program saw a 30% increase in follow-up rates just by switching to phone calls.
The Tech That Makes It Possible
You don’t need fancy gear. Most patients use smartphones they already own. The apps work on iOS 14+ and Android 10+, which cover 92% of phones in use today. But here’s the catch: 28% of rural Americans still lack broadband that meets FCC standards. And 34% of seniors say they struggle to use the apps. That’s why successful programs don’t just hand out an app and walk away. They train patients. The average patient needs two to four sessions to feel confident. Older adults need an average of 3.2 sessions. Nurses spend 47 minutes per person during setup-teaching how to use the device, how to interpret the data, and when to call for help. Security matters too. All video platforms use end-to-end AES-256 encryption. Data is stored on HIPAA-compliant servers. No one’s listening in. No one’s selling your info.What’s Missing: The Gaps in the System
Telehealth isn’t magic. It can’t replace everything. About 22% of side effects require physical touch-like checking for swelling in the legs, feeling for lymph nodes, or listening to heart sounds. These still need in-person visits. That’s why the best programs combine remote monitoring with scheduled local check-ups. Communication gaps are another problem. A patient in West Virginia once complained their video call was too blurry to see their tremors. The provider missed a key sign of a drug reaction. That’s why some clinics now use photo uploads-patients snap a picture of a rash or swelling and send it ahead of time. And then there’s the economic side. Urban telehealth companies are expanding into rural markets. They offer cheaper, faster care. But that’s hurting local clinics. A 2022 study found that when urban providers enter a rural area, local hospital revenue drops by 15%. That means fewer staff, fewer services, and less sustainability for the very programs rural patients depend on.Who’s Leading the Way
Pharmacists are becoming the backbone of rural telehealth. The American Pharmacists Association says pharmacist-led monitoring programs achieve 89% adherence. That’s 27 points higher than standard care. At Vanderbilt University, adding pharmacists to telehealth teams cut severe side effects by 43%. The FDA just approved AI tools like IBM Watson’s MedSafety system. It scans patient-reported symptoms and lab data to predict which patients are at risk of a bad reaction-84% accuracy, according to a 2023 NEJM study. It doesn’t replace the doctor. It flags the red flags before they turn into emergencies. Pharmaceutical companies are stepping in too. Pfizer and Merck have spent $450 million since 2022 on telehealth programs for rural patients. Why? Because better adherence means fewer hospitalizations-and that’s good for patients and for their bottom line.
What Patients Say
Real people have real stories. One patient in Montana, on a blood thinner, said: “The app caught my INR climbing before I felt sick. I got a call within an hour. They adjusted my dose. I didn’t end up in the ER.” Another, from rural Alabama, said: “I used to drive 90 miles every month for my antidepressant check-up. Now I do it from my kitchen table. I’ve missed only one appointment in two years.” But not all feedback is positive. Some say it feels impersonal. Others can’t get the app to work. One woman in Ohio said: “I’m 72. I don’t know what ‘sync’ means. I gave up.” The common thread? Convenience and reduced travel are the biggest wins. Patients save an average of 72 miles per visit. That’s hours saved. Gas money saved. Stress saved.How to Make It Work in Your Community
If you’re a clinician, a caregiver, or even a patient trying to get better care:- Start with the most dangerous medications: anticoagulants, antihypertensives, and psychotropics. These account for 68% of high-risk drug use in rural areas.
- Use simple tools first: Bluetooth devices that auto-send data. No complex apps.
- Train patients in person, if possible. One-on-one help cuts failure rates in half.
- Use audio-only calls for seniors who can’t use video.
- Partner with local pharmacists. They’re the most accessible health professionals in many towns.
- Build tiered responses: call immediately for chest pain, within 24 hours for nausea, within 72 hours for mild headaches.
- Push for local reimbursement. CMS pays $51 for 20 minutes of remote monitoring. But only 63% of private insurers follow that rate. Advocate for change.
The Future Is Here-But It’s Not Equal Yet
Telehealth for side effect monitoring isn’t the future. It’s happening now. In 2023, 47% of rural clinics use it. By 2025, 92% plan to expand. But progress isn’t automatic. Black rural patients are 1.8 times less likely to get these services than white patients. Broadband gaps still leave entire counties offline. Staffing shortages mean nurses are stretched too thin. The solution isn’t just better tech. It’s better policy. Fairer pay. Local investment. Community trust. For rural patients, telehealth isn’t about convenience. It’s about survival. The right system can catch a dangerous side effect before it’s too late. It can keep someone out of the hospital. It can let them stay in their home, in their community, with dignity. It’s not perfect. But it’s better than nothing. And with the right support, it can be everything.
Ian Glover
My name is Maxwell Harrington and I am an expert in pharmaceuticals. I have dedicated my life to researching and understanding medications and their impact on various diseases. I am passionate about sharing my knowledge with others, which is why I enjoy writing about medications, diseases, and supplements to help educate and inform the public. My work has been published in various medical journals and blogs, and I'm always looking for new opportunities to share my expertise. In addition to writing, I also enjoy speaking at conferences and events to help further the understanding of pharmaceuticals in the medical field.
12 Comments
-
Noah Raines
December 11, 2025 AT 15:23this is literally the only thing keeping me alive in this damn backwater town. i’m on warfarin and if i didn’t have that INR monitor, i’d be dead by now. they called me within 20 mins when my numbers spiked last month. paramedics were at my door in 40.
also side note: the pharmacist who calls me? she remembers my dog’s name. that’s more than my old doc ever did. 🙌 -
Katherine Rodgers
December 12, 2025 AT 17:22oh wow. so we’re just gonna ignore that 34% of seniors can’t use the apps? and the fact that half the rural counties don’t even have internet?
this is tech bros pretending to save lives while ignoring the fact that most of these people still use flip phones and think ‘sync’ is a type of yoga. nice marketing. -
Lauren Dare
December 14, 2025 AT 14:24let’s be real: the ‘telehealth revolution’ is just corporate cost-shifting. why pay for local nurses when you can outsource to a call center in India and charge medicare $51 for a 20-min call?
the real win? fewer hospitalizations = higher profits for pharma. the real loss? community trust. and dignity. and actual human contact.
also, ‘end-to-end AES-256 encryption’ sounds impressive until you realize grandma still sends her rash pics via facebook messenger. -
Lola Bchoudi
December 16, 2025 AT 04:24if you’re implementing this, start with anticoagulants and psychotropics-they’re the biggest killers. use bluetooth devices that auto-upload. don’t make them download apps. give them a printed QR code they can scan with their phone camera.
train them in person, even if it’s just 15 mins at the post office. pair it with weekly audio check-ins. and PLEASE partner with the local pharmacist-they’re the only ones who show up every day.
also: tiered responses are non-negotiable. chest pain = immediate call. nausea = 24 hrs. headache = 72 hrs. structure saves lives. -
Graham Abbas
December 17, 2025 AT 09:34there’s something deeply poetic about technology becoming the bridge between isolation and survival. we’ve built satellites to map distant galaxies, yet we’re only now realizing that a simple Bluetooth cuff can keep a woman in Montana from bleeding out in her kitchen.
this isn’t just healthcare. it’s an act of quiet rebellion against neglect. the fact that it works at all is a miracle. the fact that it’s not universal? that’s the tragedy. -
Haley P Law
December 17, 2025 AT 14:59i just cried reading this. my dad’s on a blood thinner and he used to drive 120 miles every 2 weeks. last month he missed his appointment because the road was washed out.
we got him the yosi cuff. he’s been using it for 3 weeks. he didn’t tell me he was scared. but i found him last night holding the device like it was a baby.
he said, ‘it’s like someone’s watching.’
they are. and that’s everything. -
Andrea DeWinter
December 17, 2025 AT 21:16for folks struggling with the tech: start simple. use your phone’s built-in camera to take pictures of rashes or swelling. send them to your nurse via text. no app needed.
if you can’t do video? phone calls work. medicare pays for them now. ask your pharmacist to call you. they’re used to it.
and if you’re a clinician? stop assuming everyone knows what ‘INR’ means. explain it like you’re talking to your grandma. she’s not dumb. she just never learned the lingo. -
Asset Finance Komrade
December 19, 2025 AT 14:29while the empirical data suggests efficacy, one must interrogate the ontological implications of remote monitoring as a proxy for care.
is a blood pressure reading truly indicative of human suffering? does algorithmic flagging replace embodied empathy?
and while IBM Watson claims 84% accuracy, it cannot comprehend the silence of a man who refuses to admit he’s afraid.
also, emojis are overrated. 🤷♂️ -
Stacy Tolbert
December 21, 2025 AT 08:55i hate to say it but… this is why i stopped trusting doctors. you tell me telehealth is saving lives, but my cousin died last year because her nurse didn’t call back for 3 days. she had chest pain. they said ‘it’s probably just anxiety’.
now i’m terrified to use any of this. what if the next time i need help, no one’s listening?
i just want someone to look me in the eye and say ‘i’ve got you’. -
Rich Paul
December 22, 2025 AT 16:15yo so the whole 'pharmacists are the backbone' thing? yeah that's cute. but did you know most of them are overworked and get paid like $20/hr to do this?
and the AI? IBM Watson? lol. it's trained on urban data. it doesn't know what 'frontier county' means.
also 47 mins per person for setup? that's not scalable. that's a luxury. most clinics have 1 nurse for 300 patients.
this whole thing is a shiny object distraction from real funding issues. fix the damn roads and hire more staff. -
Delaine Kiara
December 24, 2025 AT 15:45i’m 68. i’ve been on blood pressure meds for 15 years. i tried the app. i tried the cuff. i tried the phone call.
the app crashed. the cuff didn’t sync. the phone call? they kept putting me on hold.
so i stopped.
now i just drive 90 miles every month. it’s easier. i know the people there. they know me. they remember my dog.
i don’t need tech. i need a person who looks me in the eye and says ‘you’re doing okay’.











Write a comment
More Articles
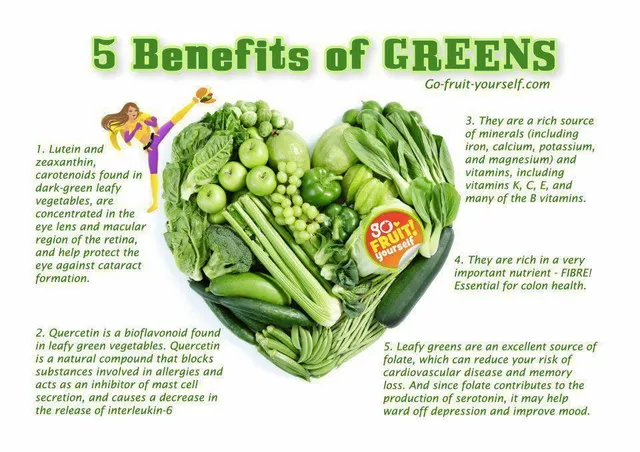
Folate Deficiency and Eye Health: What You Need to Know
As a blogger, I recently came across an important topic concerning eye health - folate deficiency. Folate, also known as vitamin B9, plays a crucial role in maintaining our overall well-being, including our precious eyesight. A deficiency in folate can lead to various eye problems, such as macular degeneration and optic neuropathy. To prevent these issues, it's essential to consume a balanced diet rich in leafy greens, beans, and fortified cereals. So, let's take care of our eyes by ensuring we get enough folate in our daily diets!
Dong Quai and Warfarin: What You Need to Know About the Bleeding Risk
Dong Quai and warfarin together can dangerously increase bleeding risk. Learn why this herbal supplement is unsafe for anyone on blood thinners, what the science says, and what to do instead.
Ampicillin and biofilms: Can it help break down bacterial communities?
In my latest research, I came across an interesting topic about Ampicillin and its potential role in breaking down bacterial communities known as biofilms. Biofilms are notorious for their resistance to antibiotics, making infections difficult to treat. Ampicillin, a widely used antibiotic, has shown some promise in disrupting these communities. Studies have suggested that it could weaken the biofilm structure, making it easier for other antibiotics to penetrate and eliminate the bacteria. It's fascinating to think that a common antibiotic like Ampicillin might be the key to tackling these stubborn bacterial communities!
Iris Carmen
December 10, 2025 AT 08:41i just got my bp cuff from yosi last month and honestly it’s been a game changer. no more driving 45 mins just to check if my meds are working. i even showed my mom how to use it and she’s 71 and she figured it out in like 10 mins.
also the text reminders? genius. i forgot my pill twice last week and got a text before i even realized. no shame.