
Ever wondered why two men with low testosterone can feel completely different? The answer often lies in the hypogonadism types they have. Knowing whether the problem starts in the testicles or higher up in the brain can change everything from testing to treatment.
Key Takeaways
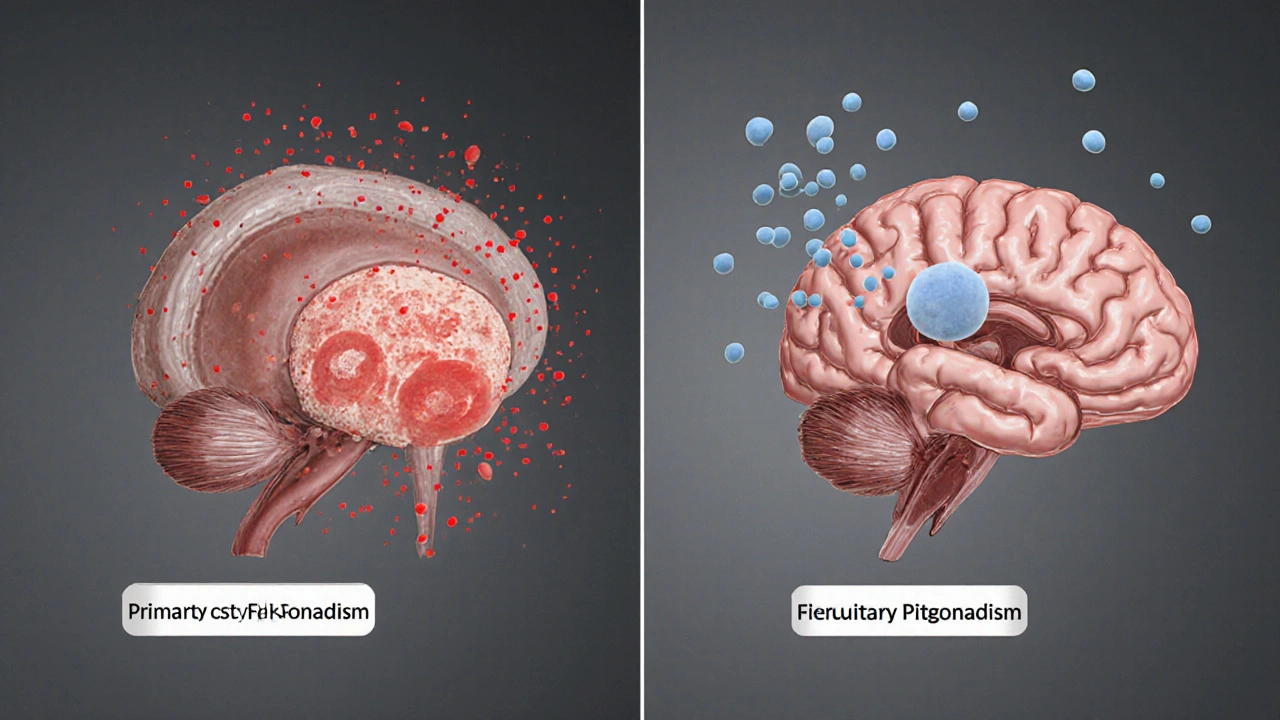
- Hypogonadism is a hormone deficiency that can originate in the testes (primary) or in the brain’s pituitary/hypothalamic axis (secondary).
- Primary and secondary forms have distinct causes, lab patterns, and treatment pathways.
- Accurate diagnosis relies on measuring testosterone together with gonadotropins - luteinizing hormone (LH) and follicle‑stimulating hormone (FSH).
- Genetic syndromes like Klinefelter and Turner are classic examples of primary hypogonadism.
- Pituitary tumors, prolonged steroid use, and high‑dose opioids are leading culprits of secondary hypogonadism.
What is Hypogonadism a condition where the body produces insufficient sex hormones, mainly testosterone in men, due to problems with the gonads or the signaling centers in the brain?
In simple terms, hypogonadism means the body’s hormone factory isn’t churning out enough testosterone. Testosterone drives muscle mass, libido, bone density, mood, and red blood cell production. When levels dip, you might notice fatigue, reduced sexual drive, loss of muscle, or even anemia.
The condition isn’t one‑size‑fits‑all. The root cause determines the label, the lab clues, and the best way to fix it.
Primary (Testicular) Hypogonadism also called hypergonadotropic hypogonadism; the testes themselves are damaged or underdeveloped, leading to low testosterone despite high stimulating hormones
With primary hypogonadism, the testicles can’t respond to signals from the brain. The pituitary gland notices the low testosterone and cranks up production of LH and FSH, so blood tests typically show high gonadotropins.
Common causes include:
- Genetic disorders - Klinefelter syndrome a male chromosomal condition (47,XXY) that impairs testicular development
- Physical injury or surgery affecting the testes
- Infections such as mumps orchitis
- Radiation or chemotherapy that damages germ cells
- Autoimmune orchitis
Secondary (Pituitary‑Hypothalamic) Hypogonadism also known as hypogonadotropic hypogonadism; the brain’s signaling centers fail to stimulate the testes, resulting in low testosterone with low or normal LH and FSH
Here the problem isn’t the testicles but the command center - the hypothalamus and pituitary gland. If they don’t release enough gonadotropins, the testes stay idle.
Typical triggers are:
- Pituitary tumor a benign growth that can compress or disrupt hormone‑secreting cells
- Prolonged use of glucocorticoids or high‑dose opioids
- Severe systemic illness (e.g., HIV, chronic kidney disease)
- Congenital defects affecting the hypothalamus - Kallmann syndrome a rare condition where the hypothalamus lacks gonadotropin‑releasing hormone (GnRH) neurons
- Trauma or surgery to the brain or pituitary stalk
Mixed or Combined Forms
Sometimes both the testes and the brain are partially impaired. Mixed hypogonadism can arise after chemotherapy that damages testicular cells while also disrupting the hypothalamic‑pituitary axis. Lab values may show intermediate or fluctuating LH/FSH levels, so a comprehensive endocrine work‑up is crucial.
How Doctors Diagnose the Different Types
The diagnostic roadmap starts with a detailed history and physical exam, followed by targeted labs:
- Morning total Testosterone the primary male sex hormone; low levels (<300 ng/dL) suggest hypogonadism measured before 10am.
- Serum Luteinizing hormone (LH) stimulates testosterone production in Leydig cells and Follicle‑stimulating hormone (FSH) supports sperm production in Sertoli cells. High levels point to primary hypogonadism; low/normal levels hint at secondary.
- Prolactin level - elevated prolactin can suppress GnRH and mimic secondary hypogonadism.
- Sex hormone‑binding globulin (SHBG) and free testosterone - useful when total testosterone is borderline.
- Imaging: MRI of the pituitary for suspected tumors; scrotal ultrasound for testicular atrophy or lesions.
- Genetic testing when a syndrome is suspected (e.g., karyotype for Klinefelter, sequencing for Kallmann).
Interpreting the hormone panel in context is the key to labeling the correct type.
Treatment Strategies Tailored to the Type
Once the type is clear, therapy becomes more focused.
- Primary hypogonadism: Direct testosterone replacement (gels, patches, injections) is usually first‑line because the testes can’t produce enough on their own. In younger men desiring fertility, gonadotropin therapy (hCG ± FSH) can stimulate natural testosterone and sperm production.
- Secondary hypogonadism: Treat the underlying cause whenever possible - surgery for a pituitary adenoma, tapering off opioids, or correcting hyperprolactinemia with dopamine agonists. If the axis remains suppressed, testosterone replacement is added, but gonadotropin therapy may be more physiological if fertility is a goal.
- Mixed cases: A combination approach-address any reversible brain factors, then supplement testosterone while monitoring testicular response.
Monitoring involves repeat hormone panels every 3‑6months, symptom questionnaires, bone density scans, and semen analysis if fertility matters.

Comparison Table: Primary vs. Secondary Hypogonadism
| Feature | Primary (Testicular) | Secondary (Pituitary‑Hypothalamic) |
|---|---|---|
| Site of defect | Testes | Hypothalamus or pituitary gland |
| LH & FSH levels | High (hypergonadotropic) | Low or normal (hypogonadotropic) |
| Common causes | Klinefelter syndrome, orchitis, radiation | Pituitary adenoma, opioids, Kallmann syndrome |
| Treatment focus | Testosterone replacement or gonadotropins for fertility | Address underlying brain issue; testosterone if needed |
| Typical age of presentation | Adolescence to late adulthood | Can appear at any age, often linked to medication or disease |
Practical Checklist for Patients and Clinicians
- Document symptoms: fatigue, libido, muscle loss, mood changes.
- Order morning total testosterone, LH, FSH, prolactin.
- If testosterone < 300ng/dL, repeat test to confirm.
- Interpret LH/FSH pattern to decide primary vs. secondary.
- Consider MRI of pituitary if secondary signs appear.
- Screen for genetic syndromes when testicular atrophy or atypical features are present.
- Discuss fertility goals early; choose hCG/FSH or testosterone accordingly.
- Set follow‑up schedule: labs every 3-6months, symptom review each visit.
Frequently Asked Questions
Can lifestyle changes reverse hypogonadism?
In secondary hypogonadism caused by obesity, excessive alcohol, or chronic stress, weight loss, better sleep, and reduced alcohol can improve hormone levels. However, structural damage to the testes or a tumor usually requires medical intervention.
Is testosterone therapy safe for older men?
Short‑term therapy is generally well‑tolerated, but clinicians monitor hematocrit, prostate‑specific antigen, and cardiovascular risk. The decision balances symptom relief with potential side effects.
What’s the difference between total and free testosterone?
Total testosterone includes the hormone bound to SHBG and albumin, while free testosterone is the biologically active fraction. In cases of abnormal SHBG (e.g., thyroid disease), free testosterone gives a clearer picture.
Can men with primary hypogonadism ever father children?
Yes, with gonadotropin therapy (hCG ± FSH) many men can stimulate natural testosterone production and restore sperm output, offering a more natural path to fertility than sperm banking.
Why is LH high in primary hypogonadism?
When testicular testosterone drops, the pituitary senses the gap and releases more LH to try to boost production. The testes can’t respond, so LH stays elevated.

Ian Glover
My name is Maxwell Harrington and I am an expert in pharmaceuticals. I have dedicated my life to researching and understanding medications and their impact on various diseases. I am passionate about sharing my knowledge with others, which is why I enjoy writing about medications, diseases, and supplements to help educate and inform the public. My work has been published in various medical journals and blogs, and I'm always looking for new opportunities to share my expertise. In addition to writing, I also enjoy speaking at conferences and events to help further the understanding of pharmaceuticals in the medical field.
18 Comments
-
Carlos A Colón
October 14, 2025 AT 08:34I feel you, navigating those hormone charts can be a real maze-except when you realize the pituitary is just as clueless as the testicles sometimes, lol. It’s almost funny how the body decides to play hide‑and‑seek with testosterone.
-
Aurora Morealis
October 20, 2025 AT 03:27Primary hypogonadism shows high LH and FSH while testosterone remains low.
-
Sara Blanchard
October 25, 2025 AT 22:21When we discuss these hormonal patterns, it’s vital to remember that patients from all backgrounds experience them, and cultural competence can improve diagnosis and care.
-
Anthony Palmowski
October 31, 2025 AT 16:14Wow, another comprehensive guide-yet the real issue lies in the clinical inertia, the overreliance on arbitrary cut‑offs, the endless debates about what constitutes ‘low’ testosterone, and the pharmaceutical over‑promotion that follows! Doctors must cut through the noise, scrutinize each lab, and question the motives behind every prescription!
-
Jillian Rooney
November 6, 2025 AT 11:07As an Americann we should be proud to demand better screening, not just accept the vague guidelines that leave many men suffering in silence.
-
Rex Peterson
November 12, 2025 AT 06:01The ontological distinction between organogenic and neurogenic origins of testosterone deficiency invites a deeper reflection on the hierarchical nature of physiological control, reminding us that causality in endocrinology is as much a matter of context as of biochemistry.
-
Candace Jones
November 18, 2025 AT 00:54If you’re unsure how to interpret LH and FSH levels, start by checking whether they are elevated relative to the testosterone reading; this simple step often points you toward primary versus secondary hypogonadism without unnecessary tests.
-
Robert Ortega
November 23, 2025 AT 19:47Both forms ultimately affect quality of life, so early detection matters.
-
Elizabeth Nisbet
November 29, 2025 AT 14:41Think of it as fine‑tuning a car: once you know which part is under‑performing, you can target the right fix and get your engine running smoothly again.
-
Sydney Tammarine
December 5, 2025 AT 09:34Behold, the grand tapestry of endocrine disruption-an intricate ballet of failing testes and a bewildered hypothalamus, each pirouetting in tragic harmony, utterly lost in the void of modern medicine 😐.
-
josue rosa
December 11, 2025 AT 04:27In the context of differential diagnosis, the clinician must adopt a systematic, algorithmic approach that integrates both biochemical markers and nuanced patient history. First, the morning total testosterone level should be obtained, preferably on at least two separate occasions to account for diurnal variation. Concomitantly, serum LH and FSH concentrations provide indispensable insight into the integrity of the hypothalamic‑pituitary‑gonadal axis. An elevated gonadotropin profile in the presence of low testosterone unequivocally points toward primary testicular failure. Conversely, a blunted or inappropriately normal LH/FSH response suggests secondary, central etiologies. It is also critical to assess prolactin and cortisol levels, as hyperprolactinemia and iatrogenic glucocorticoid excess can masquerade as hypogonadotropic states. Imaging studies, such as pituitary MRI, become indispensable when a structural lesion is suspected, particularly in the setting of visual field deficits. Genetic testing for Klinefelter syndrome (47,XXY) or Kallmann syndrome should be considered when the clinical picture aligns with these syndromes, especially in younger patients. Therapeutic interventions diverge markedly: primary hypogonadism often warrants testosterone replacement therapy, whereas secondary forms may respond to pulsatile GnRH or LH/FSH analogs. However, the decision to initiate hormone replacement must be tempered by a thorough risk–benefit analysis, taking into account cardiovascular, hematologic, and prostatic considerations. Patient counseling should emphasize the potential side effects, the necessity for regular monitoring, and the realistic expectations regarding symptom amelioration. Long‑term follow‑up includes periodic reassessment of hormone levels, hemoglobin/hematocrit, lipid profile, and bone mineral density. In refractory cases, multidisciplinary collaboration with endocrinology, urology, and reproductive specialists can optimize outcomes. Moreover, lifestyle modifications-exercise, weight management, and avoidance of excess alcohol or opioids-can augment therapeutic efficacy. Ultimately, a precise etiologic classification empowers clinicians to tailor interventions, thereby improving both biochemical parameters and patient‑reported quality of life.
-
Shawn Simms
December 16, 2025 AT 23:21The presented guide adheres to a logical structure; however, certain typographical inconsistencies merit correction, and the citation format should conform to the journal’s style guidelines.
-
Geneva Angeles
December 22, 2025 AT 18:14Guys, I’m thrilled you’re diving into this labyrinth of hormones-yes, it sounds intimidating, but think of the massive payoff when you finally demystify the cascade! Grab that lab data, dissect those LH spikes, and you’ll be wielding diagnostic power like a superhero armed with a stethoscope. No nonsense, just pure, unfiltered enthusiasm for turning confusion into clarity. Keep pushing, because every minute you spend mastering this knowledge translates directly into better patient outcomes.
-
Scott Shubitz
December 28, 2025 AT 13:07Look, the literature is drowning in vague definitions, and the so‑called ‘standard’ thresholds are as flimsy as wet tissue-stop buying into the hype! If you want real answers, demand precise assays and reject the marketing fluff that pharma throws at us. It’s time to cut the nonsense and get to the gritty truth of hormone biology.
-
Soumen Bhowmic
January 3, 2026 AT 08:01I totally agree that collaboration across specialties can streamline the diagnostic pathway, especially when we combine endocrinology insights with urologic perspectives, which ultimately benefits the patient.
-
Jenna Michel
January 9, 2026 AT 02:54Alright team, let’s turbo‑charge our approach-integrate evidence‑based protocols leverage pharmacogenomics and smash those outdated algorithms! Remember enthusiasm + precision = success.
-
Abby Richards
January 14, 2026 AT 21:47Your summary captures the essential distinctions clearly; great job on breaking down the complex endocrine pathways 😊👍.

















Write a comment
More Articles
Tung Seed: Everything You Need to Know About This Powerful Dietary Supplement
I recently came across a powerful dietary supplement called Tung seed, and I just had to share it with you guys! Tung seed comes from the Tung tree, native to China, and is packed with numerous health benefits. It is high in Omega-3 fatty acids, essential for a healthy heart, and also has anti-inflammatory properties. Many people use it to boost their immune system and maintain a healthy weight. If you haven't tried Tung seed yet, I highly recommend giving it a shot for a natural and effective boost to your overall health!

Kristen Woods
October 8, 2025 AT 13:41Indeed, the dichotomy between primary and secondary hypogonadism is a theatrical drama of endocrinology, each with its own cascade of hormonal missteps. The lab values, when interpreted correctly, definately reveal which organ-testis or hypothalamus-has betrayed its duty. Let us not overlook the profound impact this distinction has on therapeutic strategy.