Symptom Assessment Tool
Assess Your Symptoms
This tool helps you understand if your symptoms might indicate a condition that requires medical attention. Remember, this is not a diagnosis, but a guide to help you decide when to see a healthcare provider.
Symptom Information
Vaginal burning is a painful, stinging sensation that may be constant or triggered by touch, moisture, or certain foods. It can range from mild to severe and may disrupt daily activities.
How long have you experienced vaginal burning?
Does the burning occur during or after urination or intercourse?
Do you have chronic pelvic pain that lasts longer than six months?
Are you experiencing any of these additional symptoms?
Personalized Assessment
Key Takeaways
- Vaginal burning can be an early sign of conditions that also cause chronic pelvic pain.
- Inflammation, nerve irritation, and hormonal shifts link the two symptoms.
- Accurate diagnosis often requires ruling out infections, dermatologic disorders, and pelvic organ disease.
- Treatment combines medication, lifestyle tweaks, and targeted pelvic‑floor therapy.
- Seeing a specialist early can prevent long‑term discomfort and improve quality of life.
When a woman reports vaginal burning, the first thought is usually a yeast infection or irritation. But that sharp, stinging feeling can also be a clue that something deeper is happening in the pelvic region. Chronic pelvic pain (CPP) is defined as non‑malignant pain lasting six months or longer, affecting muscles, nerves, or organs in the lower abdomen. The two symptoms often intersect, and understanding the link helps you and your clinician target the right treatment.
Vaginal burning is a painful, burning or stinging sensation in the vaginal walls that may be constant or triggered by touch, moisture, or certain foods. It can arise from infections, dermatologic conditions, hormonal changes, or nerve irritation. The sensation can be mild or severe enough to disrupt daily activities, sexual intimacy, and sleep.
Chronic pelvic pain is pain in the lower abdomen or pelvis lasting more than six months, often without a clear, single cause. The pain may be localized or diffuse, and it can fluctuate with the menstrual cycle, bowel movements, or bladder filling. CPP affects up to 15% of women worldwide, making it a significant public‑health concern.
What Triggers Vaginal Burning?
Several common culprits can ignite a burning feeling:
- Infections: Yeast infection (Candida albicans) typically produces itching, thick discharge, and burning after intercourse or urination.
- Bacterial vaginosis: An overgrowth of anaerobic bacteria creates a fishy odor, thin gray discharge, and sometimes mild burning.
- Sexually transmitted infections (STIs) such as Trichomoniasis or herpes can cause intense burning and ulcerations.
- Dermatologic conditions: Vulvodynia is a chronic pain syndrome where even light touch feels burning, often without visible lesions.
- Hormonal shifts: Menopause, low estrogen, or hormonal contraceptives can thin the vaginal epithelium, making it more sensitive.
- Irritants: Perfumed soaps, douches, tight synthetic underwear, and certain lubricants can strip protective mucous layers.
These triggers don’t act in isolation. For example, prolonged antibiotic use can disrupt the vaginal microbiome, leading to yeast overgrowth that later fuels vulvar inflammation. That inflammation may then sensitize nearby nerves, bridging the gap to chronic pelvic pain.
Understanding Chronic Pelvic Pain
CPP is a broad umbrella that captures pain from multiple sources:
- Pelvic inflammatory disease (PID) - an infection of the upper reproductive tract often following untreated STIs.
- Endometriosis - endometrial tissue implants outside the uterus, causing cyclic or constant pain.
- Interstitial cystitis - a bladder condition that triggers burning during urination and pressure in the pelvis.
- Irritable bowel syndrome (IBS) - gut dysmotility that can radiate to pelvic muscles.
- Neuropathic pain - nerve damage or hypersensitivity after surgery, childbirth, or trauma.
Because CPP often involves overlapping organ systems, a single symptom like vaginal burning might be the tip of the iceberg.
Shared Pathophysiology: How the Two Symptoms Interact
Three major mechanisms tie vaginal burning to chronic pelvic pain:
- Inflammation: Infections or irritants cause local cytokine release. Cytokines spread to nearby nerves, lowering their pain threshold.
- Neuropathic sensitization: Repeated irritation damages small sensory fibers (C‑fibers) that innervate the vulva and pelvic floor, leading to chronic burning.
- Hormonal modulation: Estrogen deficiency thins mucosal barriers, making the vagina more vulnerable to micro‑abrasions that trigger pelvic‑floor muscle spasm.
Research from the International Urogynecology Society (2023) shows that women with vulvodynia are three times more likely to develop CPP within two years, underscoring the clinical relevance of early identification.
Common Underlying Conditions - A Comparative Look
| Condition | Typical Vaginal Burning? | Typical Chronic Pelvic Pain? | First‑line Treatment |
|---|---|---|---|
| Yeast infection | Yes - intense burning after intercourse or urination | Rare - may trigger secondary pelvic muscle tension | Topical or oral antifungals |
| Vulvodynia | Yes - constant or provoked burning without infection | Often - pelvic floor hypertonicity common | Pelvic‑floor physical therapy, topical lidocaine |
| Endometriosis | Occasional - lesions near the vaginal introitus | Yes - cyclic deep pelvic ache | Hormonal suppression, laparoscopic excision |
| Interstitial cystitis | Yes - burning during voiding may radiate outward | Yes - bladder pressure and pelvic discomfort | Pentosan polysulfate, bladder instillations |
| Pelvic inflammatory disease | Variable - may accompany discharge | Yes - constant lower‑abdominal pain | Broad‑spectrum antibiotics |

When to Seek Professional Help
Self‑care works for mild irritations, but you should book an appointment if any of the following appear:
- Burning persists for more than two weeks despite hygiene changes.
- Pain interferes with work, sleep, or sexual activity.
- Accompanying symptoms such as fever, abnormal bleeding, or discharge.
- History of recurrent urinary or reproductive infections.
During the visit, expect a comprehensive assessment:
- Medical history - menstrual cycle, sexual activity, medication use.
- Physical exam - speculum inspection, pelvic‑floor muscle tone evaluation.
- Laboratory tests - vaginal swab for fungus, bacteria, STI panels.
- Imaging if needed - ultrasound or MRI to rule out endometriosis or structural anomalies.
Urogynecologists, pelvic‑floor physiotherapists, and pain specialists often collaborate to create a personalized plan.
Management Strategies: From Relief to Recovery
Effective treatment usually blends three pillars: infection control, nerve modulation, and lifestyle modification.
1. Treat the Root Cause
If labs reveal Candida, a short course of fluconazole (single 150mg dose) often clears the infection. For bacterial vaginosis, metronidazole 500mg twice daily for seven days is standard. When an STI is identified, partner treatment prevents reinfection.
2. Calm the Nerves
Topical agents such as lidocaine 5% ointment provide temporary relief for vulvar burning. Neuropathic pain medications-gabapentin (starting 300mg at night) or duloxetine (30mg daily)-help re‑wire oversensitive nerves. In refractory cases, pelvic‑floor Botox injections can relax hypertonic muscles.
3. Lifestyle Tweaks
- Switch to fragrance‑free, pH‑balanced cleansers.
- Wear breathable cotton underwear; avoid tight leggings.
- Stay hydrated and limit caffeine, which can irritate the bladder.
- Incorporate gentle pelvic‑floor stretches or yoga under a therapist’s guidance.
- Consider estrogen creams if you’re post‑menopausal and have atrophic changes.
Regular follow‑up every 3-6 months allows adjustments based on symptom evolution.
Frequently Asked Questions
Can vaginal burning be a sign of something serious?
Yes. While many cases are benign, persistent burning can signal infections, dermatologic disorders, or early stages of chronic pelvic conditions like endometriosis. If it lasts beyond two weeks or is accompanied by fever, bleeding, or severe pain, see a clinician promptly.
Is there a direct link between vulvodynia and chronic pelvic pain?
Research shows a strong correlation. The chronic nerve irritation that creates vulvar burning often spreads to pelvic‑floor muscles, leading to ongoing pelvic discomfort. Treating one condition frequently improves the other.
Do hormonal changes during menopause cause burning?
Yes. Declining estrogen thins the vaginal lining, reduces natural lubrication, and makes the tissue more prone to irritation. Low‑dose estrogen creams or vaginal tablets can restore moisture and reduce burning.
Can diet affect vaginal burning and pelvic pain?
Certain foods-spicy dishes, citrus, alcohol, and caffeine-can exacerbate bladder irritation and vaginal sensitivity. A balanced diet rich in probiotics (yogurt, kefir) supports a healthy vaginal microbiome, potentially lowering infection risk.
When is surgery considered for chronic pelvic pain?
Surgery is a last resort, typically for proven structural issues like deep endometriosis nodules or severe pelvic organ prolapse. Minimally invasive laparoscopy or robotic surgery can remove offending tissue, but success rates vary, so conservative management is tried first.

Ian Glover
My name is Maxwell Harrington and I am an expert in pharmaceuticals. I have dedicated my life to researching and understanding medications and their impact on various diseases. I am passionate about sharing my knowledge with others, which is why I enjoy writing about medications, diseases, and supplements to help educate and inform the public. My work has been published in various medical journals and blogs, and I'm always looking for new opportunities to share my expertise. In addition to writing, I also enjoy speaking at conferences and events to help further the understanding of pharmaceuticals in the medical field.
16 Comments
-
Rhonda Ackley
October 16, 2025 AT 15:56Oh my goodness, where do I even start? The moment I read about vaginal burning linking to chronic pelvic pain, I felt like I was thrust onto a soap‑opera stage, complete with dramatic twists and heart‑wrenching revelations. First, imagine a woman walking through her day, minding her own business, only to be haunted by a relentless sting that makes every kiss feel like a brand of hot sauce. Then, picture the silent terror as months turn into years, and the pain refuses to dim, seeping into every facet of her life – work, sleep, even the simple joy of a warm bath. The article’s key takeaways sound simple, yet they mask an ocean of complexity beneath the surface; inflammation is not just a buzzword, it’s a molecular firestorm that re‑educates nerves to scream at the slightest touch. Hormonal shifts, especially the dreaded estrogen dip during menopause, act like a rogue conductor, turning a harmonious symphony into dissonant noise. And let’s not forget the psychological toll – the dread of intimacy, the whispering doubts about one’s femininity, the clandestine battles with self‑esteem. Sure, we have treatments: antifungals, pelvic‑floor therapy, gabapentin – but each comes with its own saga of side effects, appointments, and insurance hoops. The relentless loop of cause and effect feels like an endless cliffhanger, leaving us yearning for a clear resolution. In sum, this isn’t just a medical footnote; it’s a full‑blown drama that demands compassion, patience, and a multidisciplinary cast to bring the curtain down on this chronic agony.
-
Sönke Peters
October 16, 2025 AT 16:05Solid overview, especially the bit on cytokine spread. It's a good reminder to check both infection and nerve health. Stay chill and keep tracking symptoms.
-
Paul Koumah
October 16, 2025 AT 16:13Sure, just pop a pill and hope for the best.
-
Erica Dello
October 16, 2025 AT 16:21First off – "flaming" not "flamin" 😊. Also, the article mixes up "vulvodynia" with simple yeast infection – they’re not the same thing. If you’re getting a burning feeling, you need a proper swab, not just a home remedy. Lastly, remember to spell "menopause" correctly – it’s not "menopaused". Got it? 👍
-
sara vargas martinez
October 16, 2025 AT 16:30Let’s break this down methodically. First, vaginal burning isn’t a monolithic symptom; it can stem from a spectrum ranging from superficial irritants like scented soaps to deep‑seated neuropathic conditions such as vulvodynia. Second, the interplay between estrogen deficiency and mucosal thinning creates a perfect storm for micro‑abrasions, which then act as gateways for bacterial overgrowth, perpetuating the inflammatory loop. Third, chronic pelvic pain often masquerades as isolated discomfort, but a careful history will reveal patterns tied to menstrual cycles, bowel movements, or bladder filling – clues that point toward disorders like endometriosis or interstitial cystitis. Fourth, the diagnostic algorithm should be tiered: start with a thorough physical exam and targeted lab work (wet prep, pH test, cultures), then move to imaging if the clinical picture suggests structural disease. Fifth, treatment must be multimodal; antibiotics or antifungals address infectious triggers, while pelvic‑floor physiotherapy and neuromodulators such as gabapentin target the neural component. Sixth, lifestyle modifications – breathable cotton underwear, fragrance‑free cleansers, and a diet low in irritants – can dramatically reduce symptom severity. Seventh, patient education is paramount; many women endure months of embarrassment before seeking care, so clinicians should proactively discuss these issues. Eighth, follow‑up intervals of three to six months allow for therapeutic adjustments and prevent chronicity. Finally, remember that psychosocial support and counseling can alleviate the emotional burden that accompanies chronic pain. In essence, a comprehensive, patient‑centered approach is the only way to untangle the complex web linking vaginal burning to chronic pelvic pain.
-
Todd Anderson
October 16, 2025 AT 16:40While the medical exposition is thorough, it omits a crucial geopolitical nuance: Western pharmaceutical protocols often overlook traditional therapeutic practices that have served Indian women for millennia. Incorporating Ayurvedic modalities, when scientifically validated, could enhance outcomes and reduce reliance on synthetic agents. One must advocate for an integrative framework that respects both evidence‑based medicine and cultural heritage.
-
Dexter Smith
October 16, 2025 AT 16:50The article glosses over the data variability in pain scoring systems – a classic case of cherry‑picking favorable outcomes while ignoring the high placebo response rates reported in many clinical trials. Moreover, the suggested treatment ladder fails to address the socioeconomic barriers that prevent many patients from accessing pelvic‑floor physiotherapy, rendering the protocol ineffective for a significant subset of the population.
-
Cherish Capps
October 16, 2025 AT 17:00i think its really important 2 note that simple changes like switchin to cotton undies can make a big diff. also, dont be scared 2 ask ur doc about estrogen creams if u post‑menopause. u deserve comfort.
-
Amy Carpenetti
October 16, 2025 AT 17:10the link between inflammation and nerve sensitization is key. addressing both can break the pain cycle.
-
Paul Griffin
October 16, 2025 AT 17:20Excellent summary. For those initiating therapy, I recommend starting with a targeted antifungal regimen if indicated, followed by a structured pelvic‑floor rehabilitation program. Regular reassessment at six‑week intervals will help gauge efficacy and allow timely modifications.
-
Michael Tekely
October 16, 2025 AT 17:30From a clinical perspective, we need to differentiate nociceptive from neuropathic pain pathways – that’s where gabapentin or duloxetine come into play. Also, consider the role of pelvic‑floor biofeedback as a low‑risk adjunctive therapy.
-
Oscar Taveras
October 16, 2025 AT 17:40Indeed, a multidisciplinary approach is paramount, and I would add that fostering a culturally sensitive dialogue enhances patient adherence. 😊
-
katie clark
October 16, 2025 AT 17:50While the piece is informative, it scarcely delves into the epistemological underpinnings of pain perception, which, frankly, is where the true intellectual curiosity should lie.
-
Jason Layne
October 16, 2025 AT 18:00The so‑called "research" cited in the article is part of a grand scheme to monetize chronic conditions. Pharmaceutical conglomerates push the narrative of endless medication, keeping us dependent. Wake up, folks – the real cure lies in exposing their agenda.
-
Hannah Seo
October 16, 2025 AT 18:10Respectfully, the evidence presented is peer‑reviewed and reproducible. Personal conjecture does not replace scientific validation.















Write a comment
More Articles

Antiretroviral Therapy and Common Medications: High-Risk Interactions
Antiretroviral therapy saves lives, but dangerous drug interactions with common medications can cause serious harm. Learn which HIV drugs clash with statins, painkillers, and herbal supplements - and what to do about it.
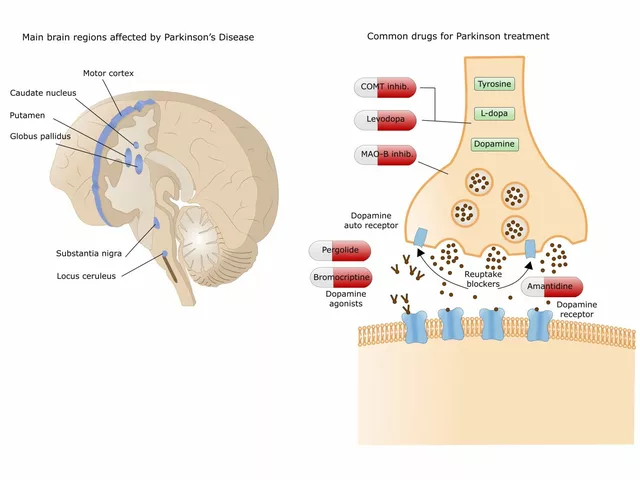
The potential benefits of betahistine for individuals with Parkinson's disease
In my recent exploration, I discovered the potential benefits of Betahistine for those living with Parkinson's disease. This medication, often used for vertigo, could potentially improve symptoms of this neurodegenerative condition. Researchers suggest that Betahistine might have the ability to reduce tremors and improve motor function. There is also a belief that it could enhance cognitive abilities and alleviate depression often associated with Parkinson's disease. However, it's important to note that more research is needed to confirm these potential benefits.

Monitoring During Immunosuppressive Therapy: Essential Lab Tests and Imaging for Safety and Effectiveness
Essential lab tests and imaging for patients on immunosuppressive therapy to prevent rejection, infection, and drug toxicity. Learn how TDM, TTV monitoring, and routine blood work keep transplant and autoimmune patients safe.
Shanmugapriya Viswanathan
October 16, 2025 AT 15:40Listen up, ladies – our Indian heritage has always known that hormonal swings can turn your vagina into a furnace 😅. Ayurvedic herbs like shatavari and neem have been used for centuries to balance estrogen and keep the mucosa supple. If you ignore those natural options, you’ll end up chasing endless pharma prescriptions. The inflammation cascade starts silently, but once the nerves are primed, the burning feels like a tiny firecracker stuck inside. So before you label it a mystery, consider diet, stress, and those time‑tested herbal allies.