When seniors experience chronic pain, opioids are sometimes the only option that works. But what many don’t realize is that what’s safe for a 40-year-old can be dangerous for someone over 65. The body changes with age-kidneys slow down, liver function declines, and fat distribution shifts. These changes mean drugs like oxycodone or morphine stick around longer and hit harder. That’s why using opioids in older adults isn’t just about picking a pill; it’s about careful, personalized planning.
Why Opioids Are Riskier for Seniors
Older adults are more likely to be on multiple medications. A typical 70-year-old might be taking blood pressure pills, diabetes drugs, antidepressants, and sleep aids. Add an opioid into that mix, and the risks climb fast. Sedation, confusion, falls, and breathing problems become real dangers. A 2023 study in JAMA Network Open found that when strict opioid limits were applied to seniors with cancer, many were switched to tramadol or gabapentin. But those alternatives? They cause dizziness and mental fog in older people, leading to more falls and hospital visits.
Then there’s the issue of metabolism. The liver and kidneys don’t clear drugs as efficiently in seniors. A standard 10 mg dose of oxycodone might be fine for a younger adult, but for someone over 75, it could be too much. That’s why guidelines now say: start at 30% to 50% of the usual adult dose. For many, that means beginning with just 2.5 mg of oxycodone or 7.5 mg of morphine-half of what’s in a standard tablet.
What Opioids Are Safe? What to Avoid
Not all opioids are created equal for seniors. Some are outright dangerous. Meperidine (Demerol) is banned for older adults because its metabolite builds up in the body and can trigger seizures and delirium. Codeine is also off-limits-many seniors lack the enzyme needed to convert it into its active form, making it useless. Others convert it too quickly, leading to overdose.
Tramadol and tapentadol? Use with caution. They carry a risk of serotonin syndrome when mixed with common antidepressants like SSRIs. That’s a rare but life-threatening condition. Methadone is another no-go. Its long half-life and unpredictable metabolism make dosing a guessing game, especially in frail seniors.
On the safer side: oxycodone, hydromorphone, and morphine can still work-if dosed properly. But the real standout is buprenorphine. It’s a partial opioid agonist, meaning it reduces pain without the same level of respiratory depression. A 2024 study in the American College of Osteopathic Family Physicians Journal showed that low-dose transdermal buprenorphine caused no central nervous system side effects when combined with small doses of oxycodone. It also caused less constipation than full opioids, which is huge-constipation is one of the most common reasons seniors stop taking pain meds.
Dosing Rules That Save Lives
There’s no one-size-fits-all dose for seniors. But there are clear rules to follow.
- Start low: Use 30-50% of the standard adult dose for opioid-naïve patients.
- Avoid patches and long-acting pills at first. These deliver steady, uncontrolled doses. If a senior’s metabolism slows unexpectedly, they can overdose.
- Use immediate-release forms first. That way, you can adjust the dose daily based on response.
- Never exceed 40 mg of morphine equivalents (MME) per day unless absolutely necessary. That’s considered a low-dose range for seniors.
- Don’t rush titration. Wait at least 48 hours between dose increases for short-acting opioids like oxycodone.
For those who need even smaller doses, liquid formulations exist. A 1 mg/mL oxycodone elixir allows for precise drops-something a 2.5 mg tablet can’t offer. Pharmacists can compound these if needed.
What About Non-Opioid Options?
Before opioids, try everything else. But not all non-opioid options are safe either.
NSAIDs like ibuprofen or naproxen? They’re risky for seniors. They can cause stomach bleeding, kidney failure, and heart attacks. Use them only for short bursts-no more than 1-2 weeks-and only if kidney function is normal.
Gabapentin and pregabalin? They’re often used for nerve pain, but studies show they only reduce pain by about 1 point on a 10-point scale. Meanwhile, they cause dizziness, confusion, and falls. The JAMA study found that after the 2016 CDC guidelines, many seniors were pushed onto these drugs instead of opioids-only to end up worse off.
Physical therapy, heat/cold therapy, acupuncture, and cognitive behavioral therapy for pain (CBT) are far safer and often more effective long-term. But they take time and commitment. That’s why opioids still have a place-for patients with cancer, severe arthritis, or post-surgical pain who need immediate relief.
Monitoring Is Not Optional
Starting an opioid is just the beginning. Monitoring is where safety happens.
The Medical Board of California requires clinicians to check in regularly: every 1-3 months at first. They look for:
- Is pain improving? Not just the number on a scale-but can the patient get out of bed? Walk to the bathroom? Sleep through the night?
- Are there signs of confusion, drowsiness, or slurred speech? These could mean opioid-induced delirium.
- Is constipation being managed? Laxatives should be prescribed from day one.
- Is the patient falling more? A simple balance test can catch rising fall risk.
- Are there signs of misuse? Urine drug screens help confirm the patient is taking what’s prescribed.
Also, never skip a treatment agreement if opioid therapy lasts longer than three months. It’s not about distrust-it’s about clarity. The patient should know the goals: "We’re aiming to help you walk to the kitchen without pain, not to eliminate every ache." That keeps expectations realistic.
What the Guidelines Got Wrong-and How They Fixed It
In 2016, the CDC released opioid guidelines meant to curb misuse. But they were applied too broadly. Doctors started refusing opioids to cancer patients, nursing home residents, and those with end-stage arthritis. The result? Untreated pain. More suffering. More emergency visits.
The 2022 CDC update corrected this. It explicitly said: "These guidelines do not apply to patients with cancer, palliative care, or end-of-life pain." It also said: "Don’t use rigid dose limits. Use clinical judgment."
That’s a game-changer. The American Geriatrics Society, the American Society of Clinical Oncology, and the National Comprehensive Cancer Network all agree: opioids are the first-line treatment for moderate-to-severe cancer pain. About 75% of patients respond well. Pain drops by half on average.
But here’s the catch: if you start too high or move too fast, you can harm someone who could have been helped. That’s why individualization matters more than ever.
What’s Next for Senior Pain Care
The future is personal. Pharmacogenetic testing-where a simple cheek swab shows how a person metabolizes drugs-is becoming more accessible. Some seniors respond poorly to oxycodone but do great with hydromorphone. Testing can tell you that before you start.
Non-drug options are expanding too. Targeted nerve blocks, spinal cord stimulators, and wearable TENS units are now covered by Medicare in more cases. Physical therapy programs designed for older adults are proving just as effective as pills for back and knee pain.
But for now, opioids still have a role. And when used right-with low doses, slow titration, close monitoring, and constant communication-they can give seniors back their independence. Not just less pain. More life.
Are opioids ever safe for seniors with dementia?
Opioids can be used cautiously in seniors with mild to moderate dementia if pain is clearly documented-like a hip fracture or severe arthritis. But they require extra monitoring because confusion can mask both pain and side effects. Never start opioids in someone with advanced dementia unless pain is confirmed through behavior changes (grimacing, refusal to move, agitation) and other causes have been ruled out. Always involve family and caregivers in decision-making.
Can I use a fentanyl patch for an elderly person?
Fentanyl patches are not recommended for opioid-naïve seniors. They deliver a constant, high dose over 72 hours. If the person’s metabolism slows or they become dehydrated, the drug builds up dangerously. Fentanyl patches should only be used after the patient has already been stabilized on oral opioids for at least a week and has shown tolerance. Even then, start with the lowest available patch (12 mcg/hour) and monitor closely.
Why is constipation such a big deal with opioids in seniors?
Constipation affects nearly all seniors on opioids. But in older adults, it’s not just uncomfortable-it’s dangerous. Severe constipation can lead to bowel obstruction, urinary retention, and even delirium. It also causes falls if the person strains too hard. That’s why laxatives (like polyethylene glycol or senna) are prescribed from day one. Stool softeners alone aren’t enough. Regular bowel routines, hydration, and fiber are essential too.
Is tramadol really unsafe for seniors?
Tramadol isn’t banned, but it’s risky. It’s metabolized by the liver into a stronger opioid, and many seniors have reduced liver function. It also increases serotonin levels, which can cause dangerous interactions with antidepressants. Studies show it causes more dizziness and falls than other opioids in older adults. It’s also less effective for moderate-to-severe pain. Most experts now reserve tramadol for very mild pain and only if no other options exist.
How often should seniors on opioids have blood tests?
Routine blood tests aren’t required for most seniors on opioids. But kidney and liver function should be checked before starting and then every 3-6 months, especially if the patient is over 80 or has existing kidney disease. If the patient is on long-term therapy, annual liver panels and electrolyte checks help catch early signs of toxicity. Urine drug screens are more useful than blood tests-they confirm adherence and detect undisclosed medications.

Ian Glover
My name is Maxwell Harrington and I am an expert in pharmaceuticals. I have dedicated my life to researching and understanding medications and their impact on various diseases. I am passionate about sharing my knowledge with others, which is why I enjoy writing about medications, diseases, and supplements to help educate and inform the public. My work has been published in various medical journals and blogs, and I'm always looking for new opportunities to share my expertise. In addition to writing, I also enjoy speaking at conferences and events to help further the understanding of pharmaceuticals in the medical field.
11 Comments
-
Gouris Patnaik
February 8, 2026 AT 07:20India has been managing elderly pain for centuries without opioids. We use ashwagandha, ginger paste, and silence. You Westerners overmedicate because you fear discomfort. Pain is not an enemy - it’s a teacher. Your body is trying to tell you to slow down, to meditate, to stop scrolling. Instead, you reach for a pill. This isn’t healthcare - it’s spiritual laziness.
-
Jesse Lord
February 8, 2026 AT 16:13My grandma was on oxycodone for 3 years after her hip replacement. Started at 2.5 mg, stayed there. No falls, no confusion, just better mornings. She’d make pancakes and watch her grandkids play. That’s the goal - not zero pain, but enough to live. I’ve seen too many docs treat seniors like broken machines. You don’t fix pain with rigid rules. You fix it with patience and listening.
-
Ashley Hutchins
February 9, 2026 AT 04:43Why are we even talking about this like its a science experiment? Opioids are a gateway to addiction and the government knows it. My neighbor’s husband died from a fentanyl patch - they said it was ‘accidental’ but he never even had surgery. This whole system is rigged. People are being drugged to keep them docile. And now they’re pushing buprenorphine like its some miracle cure? Please. Wake up. It’s all the same poison with a new label.
-
Amit Jain
February 10, 2026 AT 04:57Bro this is the dumbest thing I’ve read all week. You say start at 30% of the dose but then you list 10mg oxycodone as normal? That’s not normal - that’s a death sentence. And you call tramadol risky? Try giving it to a 78-year-old on Zoloft. I’ve seen three people in my village go into serotonin storm. One of them peed himself for three days. You think constipation’s bad? Try explaining to a widow why her husband’s brain turned to mush because some doctor thought he was ‘safe’.
-
Eric Knobelspiesse
February 10, 2026 AT 05:05So the real issue isn’t opioids - its that we treat seniors like they’re just old people and not humans with complex biology. You know what’s wild? The same docs who say ‘don’t use fentanyl patches’ will prescribe 100mg gabapentin for nerve pain. That’s 4x the max recommended dose. We’re just swapping one risk for another because we’re too lazy to do real assessment. And don’t even get me started on urine screens being used as punishment instead of communication. We need more empathy and less algorithm.
-
Catherine Wybourne
February 11, 2026 AT 14:11My mum in London was on morphine for pancreatic pain. She was 82. We did everything right - low dose, liquid form, laxatives from day one. She could still hug us. That’s the win. But what kills me is how often doctors skip the human part. They don’t ask: ‘Can you still smell the roses?’ or ‘Do you still laugh at silly cat videos?’ Pain isn’t a number on a scale. It’s the silence between laughs. The weight of a hand holding yours. If opioids help with that - use them. Carefully. But use them.
-
Mayank Dobhal
February 11, 2026 AT 18:50Tramadol is trash. Full stop.
-
Natasha Bhala
February 13, 2026 AT 17:45My aunt’s on buprenorphine patch now. She’s 81. No constipation. No fog. Just walks her dog every morning. I cried. I didn’t know pain meds could feel like this. Thank you for writing this.
-
Mary Carroll Allen
February 14, 2026 AT 06:42Wait so if someone has dementia and can’t say they’re in pain… we just let them suffer? That’s not ethical. I work in a nursing home. We had a woman who stopped eating because her hip hurt. No one knew. We had to watch her decline for weeks. Opioids saved her life. Not because they’re perfect - but because silence isn’t consent. We owe people dignity. Even when they can’t speak.
-
Joey Gianvincenzi
February 16, 2026 AT 02:01It is imperative to underscore that the ethical imperatives governing opioid administration in geriatric populations must be anchored in rigorous clinical protocol, not anecdotal extrapolation. The utilization of pharmacogenetic testing, while promising, remains insufficiently validated in longitudinal cohorts. One must not conflate anecdotal efficacy with population-wide therapeutic validity. Furthermore, the normalization of liquid formulations as a panacea ignores regulatory variance across jurisdictions. A standardized, evidence-based, multidisciplinary approach remains non-negotiable.










Write a comment
More Articles

The Role of Azilsartan in Treating Hypertension in Pregnant Women
As a copywriter, I've recently come across the topic of Azilsartan and its role in treating hypertension in pregnant women. It's interesting to know that this medication can help manage high blood pressure during pregnancy, ensuring the well-being of both mother and baby. It's essential to maintain a healthy blood pressure, as uncontrolled hypertension could lead to complications such as preeclampsia. However, it's important to consult with a healthcare professional before taking Azilsartan, as they will be able to determine if it's the right treatment option. Overall, Azilsartan seems to be a promising solution for managing hypertension in pregnant women, contributing to healthier pregnancies.
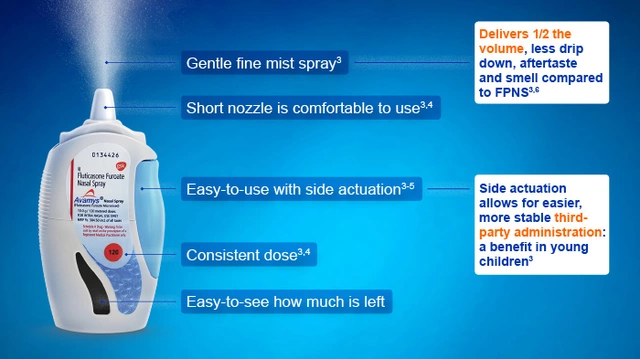
Fluticasone for Travelers: Managing Allergies on the Go
As a traveler, I've found that fluticasone is a game changer in managing allergies on the go. This nasal spray helps reduce inflammation and control common allergy symptoms, allowing me to fully enjoy my trips without constantly sneezing or dealing with itchy eyes. It's easy to pack and use, making it a must-have in my travel essentials. I highly recommend fluticasone for fellow travelers who suffer from allergies, as it makes exploring new places so much more enjoyable. Remember to consult with your doctor before using any medication, especially if you're planning an adventure abroad!

Safe Allergy Medications During Pregnancy: What You Need to Know
Managing allergies during pregnancy requires careful medication choices. Safe options include nasal steroids like Rhinocort and second-gen antihistamines like Zyrtec. Avoid decongestants like Sudafed in the first trimester. Non-drug methods like saline rinses help reduce symptoms. Always consult your doctor before taking any medication.
Patrick Jarillon
February 8, 2026 AT 02:12Let me guess - this whole thing was written by Big Pharma shills. Opioids? They’re not dangerous, they’re a government mind-control tool disguised as pain relief. Did you know the FDA approved morphine in 1903 to pacify rebellious farmers? Yeah, it’s all connected. I’ve got sources. I’ve got spreadsheets. I’ve got a cousin who works at a compounding pharmacy in Belfast. You think your 2.5 mg dose is safe? Try 0.7 mg. Or better yet - just drink turmeric tea and scream into a pillow. That’s real medicine.