Key Takeaways
- headache types fall into primary (migraine, tension, cluster, sinus, medication‑overuse) and secondary categories.
- Location, pain quality, duration, and associated symptoms help you pinpoint the exact type.
- Lifestyle tweaks (hydration, sleep hygiene, stress management) prevent many everyday attacks.
- Over‑the‑counter pain relievers work for occasional tension aches, but recurring pain often needs prescription or preventive therapy.
- Seek urgent medical care if pain is sudden, severe, or accompanied by neurological signs.
What is a Headache and Why Does It Matter?
A headache is not a disease itself; it’s a signal that something in the nervous system or surrounding structures is off‑balance. The brain itself lacks pain receptors, so the pain originates from the meninges, blood vessels, muscles, or nerves around the skull. Understanding the source helps you choose the right remedy instead of blindly popping pills.
Primary vs. Secondary Headaches
Doctors split headaches into two broad buckets:
- Primary headaches are standalone conditions-migraine, tension‑type, cluster, sinus, and medication‑overuse headaches. They aren’t caused by another disease.
- Secondary headaches signal an underlying issue such as infection, head injury, vascular problems, or medication side‑effects.
Most people experience primary headaches, but recognizing red‑flag symptoms that point to a secondary cause can be lifesaving.
Common Primary Headache Types
Below are the six most frequently diagnosed primary headaches, each with its own hallmark features.
tension headache
Also called a stress headache, this is the most common type. The pain feels like a tight band around the head, often dull and bilateral. Triggers include prolonged screen time, poor posture, and emotional stress. Episodes last from 30 minutes to several days and usually improve with rest, hydration, or simple over‑the‑counter analgesics.
migraine
Migraines are intense, pulsating headaches lasting 4-72 hours. They’re usually unilateral (one side) and can be accompanied by nausea, vomiting, and sensitivity to light or sound. About 25% of migraine sufferers experience an aura-visual disturbances like flashing lights or zig‑zag lines-before the pain starts. Triggers are diverse: hormonal fluctuations, certain foods (aged cheese, chocolate), lack of sleep, and environmental changes.
cluster headache
Cluster headaches are rare but excruciating. They strike in cycles (clusters) that can last weeks to months, followed by remission periods. Pain is severe, orbital (around one eye), and often associated with tearing, nasal congestion, or drooping eyelid on the affected side. Episodes can occur up to eight times a day, each lasting 15‑180 minutes. Smoking and alcohol are strong triggers during a cluster period.
sinus headache
Sinus headaches stem from inflammation of the sinus cavities, usually due to infection or allergies. Pain is deep‑sitting, worsens with bending forward, and is often paired with facial pressure, nasal discharge, and fever. Over‑the‑counter decongestants or antibiotics (if bacterial) resolve most cases.
medication‑overuse headache
Paradoxically, using pain relievers too often can trigger a chronic daily headache. If you take triptans, NSAIDs, or ergotamines on more than 10‑15 days per month, the brain becomes sensitized and pain recurs even without a new trigger. The cure is a structured withdrawal protocol under a physician’s supervision, followed by preventive therapy.
secondary headache
Secondary headaches arise from another medical condition-think concussion, meningitis, temporal arteritis, brain tumor, or high blood pressure. Because the underlying cause varies widely, treatment focuses on addressing that primary issue. Red‑flag signs that demand urgent evaluation include sudden “worst ever” pain, fever, neck stiffness, altered consciousness, or new neurological deficits.

How to Differentiate Headache Types
Doctors use a simple checklist to narrow down the diagnosis. Ask yourself these questions:
- Where is the pain located? (front, side, behind the eyes, whole head)
- How would you describe the pain? (throbbing, pressure, burning)
- How long does an episode last?
- What, if anything, triggers the attack?
- Are there accompanying symptoms-nausea, visual changes, nasal discharge, eyelid droop?
- How often does it happen? (sporadic vs. daily)
Matching your answers to the patterns above usually points to the right category.
Comparison Table of Primary Headaches
Key differences among primary headache types
Headache Type
Typical Pain Location
Quality & Duration
Common Triggers
First‑Line Treatment
Tension
Both sides, band‑like
Dull, 30min‑days
Stress, poor posture, fatigue
OTC NSAIDs, relaxation
Migraine
One side, often behind eye
Pulsating, 4‑72h
Hormones, certain foods, sleep changes
Triptans, anti‑emetics, preventive meds
Cluster
Orbital, unilateral
Severe, 15‑180min
Alcohol, smoking, seasonal patterns
High‑flow oxygen, sumatriptan injection
Sinus
Forehead, cheekbones
Pressure, days‑weeks
Allergies, infections
Decongestants, antibiotics if bacterial
Medication‑Overuse
Any area, often diffuse
Daily, chronic
Frequent NSAID/triptan use
Medication withdrawal, preventive therapy
When to Seek Professional Help
Most headaches are benign, but a handful of warning signs-known as "red flags"-should prompt immediate medical evaluation:
- Sudden, severe pain described as "thunderclap".
- Fever, stiff neck, or rash (possible meningitis).
- New neurological symptoms: vision loss, weakness, speech difficulty.
- Headache after head trauma, even if mild.
- Progressive worsening over weeks or months.
If any of these appear, go to an emergency department or call your doctor right away.

Management Strategies for Everyday Relief
Below are practical steps you can start using today, whether you’re dealing with occasional tension aches or chronic migraines.
Lifestyle Tweaks
- Hydration: Aim for at least 2L of water daily; dehydration is a common trigger.
- Sleep hygiene: Keep a regular 7‑9hour schedule; avoid screens 30minutes before bed.
- Screen breaks: Follow the 20‑20‑20 rule (every 20minutes, look 20feet away for 20seconds).
- Exercise: Moderate aerobic activity 3‑4 times a week reduces tension and migraine frequency.
- Stress reduction: Try mindfulness, breathing exercises, or short walks when you feel tension building.
Medication Guide
- For occasional tension headaches, ibuprofen 200‑400mg or acetaminophen works well.
- Migraine attacks often need triptans (sumatriptan, rizatriptan) taken early in the aura phase.
- Preventive meds-beta‑blockers, CGRP antagonists, or anticonvulsants-are reserved for >4 attacks per month.
- Avoid daily NSAID use beyond 10 days to prevent medication‑overuse headaches.
Non‑Pharmacologic Therapies
- Cold or warm compress: Cold for migraine throbbing, warm for tension muscles.
- Massage or physiotherapy: Relieve neck and shoulder muscle tightness.
- Acupuncture: Some studies show reduced migraine frequency.
- Cognitive‑behavioral therapy (CBT): Helps manage stress‑related tension headaches.
Preventive Checklist
Keep this quick list handy to stop headaches before they start:
- Track triggers in a diary (food, sleep, stress).
- Maintain consistent meal times; avoid skipping meals.
- Limit caffeine to ≤200mg per day.
- Wear sunglasses outdoors to reduce glare‑induced migraines.
- Schedule regular eye exams-uncorrected vision strain can mimic tension pain.
Frequently Asked Questions
What is the difference between a migraine and a tension headache?
Migraine pain is usually throbbing, one‑sided, lasts longer (4‑72hours), and comes with nausea, light and sound sensitivity, or an aura. Tension headache pain feels like a steady pressure across both sides, lasts from half an hour to a few days, and rarely includes nausea or visual changes.
When should I see a doctor for a headache?
Seek medical care if the headache is sudden and severe, accompanied by fever or neck stiffness, causes visual loss or weakness, follows a head injury, or changes dramatically in pattern. Also, if you need medication more than 10 days a month, get evaluated for medication‑overuse headache.
Can dietary changes help prevent migraines?
Yes. Many migraine sufferers find relief by avoiding trigger foods such as aged cheeses, processed meats, chocolate, and excessive caffeine. Keeping a food‑symptom diary helps pinpoint personal culprits.
What are the best over‑the‑counter options for a tension headache?
Ibuprofen 200‑400mg or naproxen 220mg taken with food works well for most people. If you can’t tolerate NSAIDs, acetaminophen 500‑1000mg is a safe alternative.
Is it safe to use triptans daily for chronic migraine?
No. Triptans are meant for acute attacks and can cause medication‑overuse headaches if used more than 10 days per month. For chronic migraine, doctors usually prescribe preventive medications or newer CGRP‑targeted therapies.
Next Steps
If you’ve identified a pattern that matches migraine or cluster headaches, book an appointment with a neurologist for a full assessment. For occasional tension or sinus pain, try the lifestyle tweaks and OTC options listed above for a week-if relief doesn’t happen, bring your symptom diary to a primary‑care doctor for further work‑up.
Remember, a headache is your body’s way of telling you something needs attention. By knowing the type, triggers, and proper treatment, you turn that warning into a manageable part of life rather than a constant mystery.
| Headache Type | Typical Pain Location | Quality & Duration | Common Triggers | First‑Line Treatment |
|---|---|---|---|---|
| Tension | Both sides, band‑like | Dull, 30min‑days | Stress, poor posture, fatigue | OTC NSAIDs, relaxation |
| Migraine | One side, often behind eye | Pulsating, 4‑72h | Hormones, certain foods, sleep changes | Triptans, anti‑emetics, preventive meds |
| Cluster | Orbital, unilateral | Severe, 15‑180min | Alcohol, smoking, seasonal patterns | High‑flow oxygen, sumatriptan injection |
| Sinus | Forehead, cheekbones | Pressure, days‑weeks | Allergies, infections | Decongestants, antibiotics if bacterial |
| Medication‑Overuse | Any area, often diffuse | Daily, chronic | Frequent NSAID/triptan use | Medication withdrawal, preventive therapy |
What is the difference between a migraine and a tension headache?
Migraine pain is usually throbbing, one‑sided, lasts longer (4‑72hours), and comes with nausea, light and sound sensitivity, or an aura. Tension headache pain feels like a steady pressure across both sides, lasts from half an hour to a few days, and rarely includes nausea or visual changes.
When should I see a doctor for a headache?
Seek medical care if the headache is sudden and severe, accompanied by fever or neck stiffness, causes visual loss or weakness, follows a head injury, or changes dramatically in pattern. Also, if you need medication more than 10 days a month, get evaluated for medication‑overuse headache.
Can dietary changes help prevent migraines?
Yes. Many migraine sufferers find relief by avoiding trigger foods such as aged cheeses, processed meats, chocolate, and excessive caffeine. Keeping a food‑symptom diary helps pinpoint personal culprits.
What are the best over‑the‑counter options for a tension headache?
Ibuprofen 200‑400mg or naproxen 220mg taken with food works well for most people. If you can’t tolerate NSAIDs, acetaminophen 500‑1000mg is a safe alternative.
Is it safe to use triptans daily for chronic migraine?
No. Triptans are meant for acute attacks and can cause medication‑overuse headaches if used more than 10 days per month. For chronic migraine, doctors usually prescribe preventive medications or newer CGRP‑targeted therapies.

Ian Glover
My name is Maxwell Harrington and I am an expert in pharmaceuticals. I have dedicated my life to researching and understanding medications and their impact on various diseases. I am passionate about sharing my knowledge with others, which is why I enjoy writing about medications, diseases, and supplements to help educate and inform the public. My work has been published in various medical journals and blogs, and I'm always looking for new opportunities to share my expertise. In addition to writing, I also enjoy speaking at conferences and events to help further the understanding of pharmaceuticals in the medical field.
14 Comments
-
Anthony Aspeitia-Orozco
October 19, 2025 AT 19:15Reading through this guide reminded me how interconnected our daily habits are with the way our brains signal pain. When you pause to consider why a particular trigger repeats, you start to see patterns that are almost philosophical. I encourage you to keep a simple diary-note sleep, water, stress, and food, then look for the recurring themes. Over time the diary becomes a mentor, gently pointing you toward the changes that matter most. Remember, adjusting one small habit can ripple into a noticeably calmer mind.
-
Robert Brown
October 26, 2025 AT 16:55This guide is fluff; skip the tables and just take ibuprofen.
-
Warren Nelson
November 2, 2025 AT 15:35Nice breakdown, especially the part about hydration-yeah, I’ve been chugging water and actually feel the tension melt a bit. The 20‑20‑20 rule is something I tried at my desk and it stops my eyes from feeling like they’re on fire. I also found that a quick walk after lunch does wonders for the “band‑like” tension. Keep the practical tips coming.
-
Jennifer Romand
November 9, 2025 AT 14:15One cannot help but be struck by the sheer audacity of presenting such a pedestrian compendium as though it were a revelation of the human condition. The language, while serviceable, lacks the lyrical gravitas befitting a discourse on cranial torment. Still, the effort to delineate each nosological entity does possess a faint glimmer of scholarly intent. One hopes future revisions shall ascend beyond mere enumeration into the realm of true enlightenment.
-
Kelly kordeiro
November 16, 2025 AT 12:55The exposition before us endeavors to unravel the labyrinthine tapestry of cephalic afflictions with an ambition most commendable. To commence, the distinction between primary and secondary headaches is not merely taxonomical but serves as the cornerstone upon which diagnostic acumen is erected. In the realm of primary headaches, the tension-type malaise presents as a bilateral constriction, reminiscent of a reluctant corset fastening the skull. Migraine, that capricious sovereign of neurologic suffering, unfurls its parasitic aura with a pulsating rhythm that belies its underlying vascular choreography. Cluster headaches, though scarce, command a ferocity akin to a meteor striking the orbital region, demanding immediate and aggressive intervention. Sinus-related pain, often masquerading as an ordinary cold, can be discerned by its exacerbation upon forward flexion and its association with mucosal secretions. The paradoxical entity of medication‑overuse headache illustrates the treacherous irony whereby therapeutic agents become the very source of chronicity. Secondary headaches, by contrast, are harbingers of deeper pathologies, ranging from infectious meningitis to the insidious progression of neoplastic processes. The author wisely enumerates red‑flag symptoms, thereby furnishing the reader with a vigilant checklist to forestall disastrous oversight. Lifestyle modulation, such as regimented hydration, calibrated sleep hygiene, and systematic stress mitigation, constitutes a non‑pharmacologic arsenal of remarkable efficacy. Moreover, the incorporation of physical modalities-warm compresses for tension, cold for migraine-embodies an integrative approach that respects the patient’s autonomy. Pharmacologic recommendations are delineated with precision, distinguishing acute agents such as triptans from prophylactic options including beta‑blockers and CGRP antagonists. The narrative further extols the virtues of adjunctive therapies, from acupuncture’s subtle needlework to the cognitive restructuring afforded by behavioral therapy. In summation, this guide traverses the intricate spectrum of cranial pain with both scholarly rigor and compassionate pragmatism. It equips the layperson with knowledge sufficient to navigate the oft‑confusing medical landscape without succumbing to panic. Simultaneously, it reminds the clinician of the necessity for discerning inquiry when confronted with atypical presentations. Thus, armed with this compendium, one may transform the daily specter of headache into a manageable, and perhaps even surmountable, facet of existence.
-
Chris Fulmer
November 23, 2025 AT 11:35I’m really glad this guide highlights the role of everyday habits in headache prevention. It’s fascinating how something as simple as consistent meal times can make a difference. Have you tried logging your caffeine intake? Some folks find that cutting back to about 200 mg a day eases both tension and migraine frequency. Keep experimenting and share what works!
-
William Pitt
November 30, 2025 AT 10:15Hey Anthony, that diary tip really resonated with me-I started a tiny spreadsheet and already spotted a pattern with late‑night screens. Thanks for the gentle nudge to treat the diary like a mentor; it’s changing the way I view my own headaches.
-
Jeff Hershberger
December 7, 2025 AT 08:55While the prose aspires to loftiness, the practical value remains marginal, leaving readers to wade through embellished verbiage for a handful of actionable tips.
-
Lawrence Jones II
December 14, 2025 AT 07:35💡 Great synthesis! The delineation of primary vs. secondary etiologies feels like a solid #clinicalalgorithm. I’d add that integrating a headache‑frequency log into a digital health app can streamline trigger correlation 📊.
-
Robert Frith
December 21, 2025 AT 06:15Honestly, all this medical mumbo‑jumbo is what keeps us from getting real, hard‑working folks back on the job-stop over‑complicating headaches and just push some ibuprofen, ya know?
-
Brad Tollefson
December 28, 2025 AT 04:55I appreciate the straightforward approach, but “mumbo‑jumbo” might be more accurately termed “complex terminology.” Nonetheless, a balanced perspective benefiits everyone.
-
Paul van de Runstraat
January 4, 2026 AT 03:35Oh sure, because if we all just pop pills like candy, the world will be headache‑free-what could possibly go wrong?
-
Lewis Lambert
January 11, 2026 AT 02:15While sarcasm adds spice, the underlying truth remains: indiscriminate analgesic use can usher in medication‑overuse headaches, a paradox that transforms relief into chronic torment. To safeguard against this, consider setting a strict limit on OTC consumption-no more than ten days per month-and consult a healthcare professional for a tailored preventive plan.













Write a comment
More Articles

How to Buy Cheap Generic Neurontin Online Safely
Learn how to safely buy cheap generic Neurontin (gabapentin) online, spot legit pharmacies, compare prices, and avoid scams with a step‑by‑step guide.
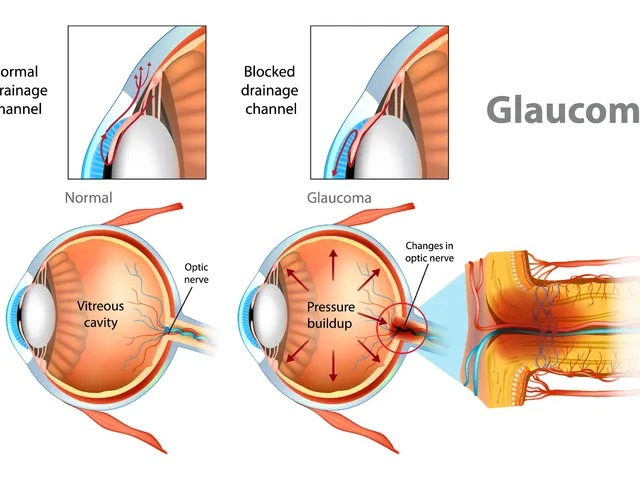
The effectiveness of dorzolamide in treating different types of glaucoma
Hey there, gentlemen! I just wanted to share some insights on a very interesting topic - the effectiveness of dorzolamide in treating different types of glaucoma. We'll dive into its mechanism of action, its beneficial effects on different types of this eye condition, and why it's becoming a go-to medication. Through this, I hope to provide everyone with a deeper understanding of this treatment option in a clear and simple language. Remember, knowledge is your best ally in health matters!
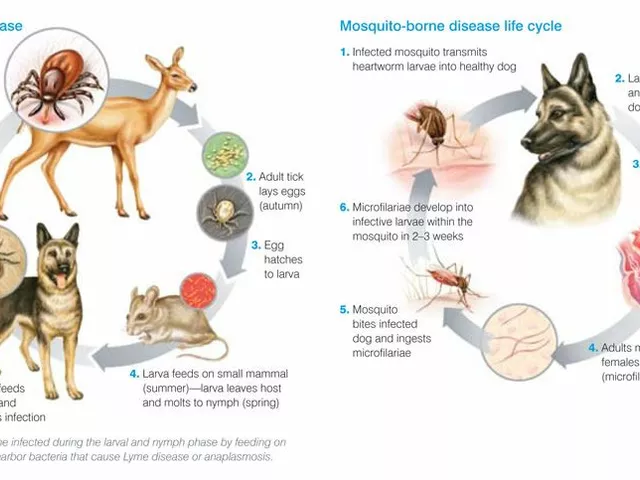
Tick Fever: What You Need to Know About This Dangerous Disease
Tick Fever, also known as Tick-Borne Disease, is a serious illness transmitted by ticks. It's crucial to be aware that this disease can have severe health implications including fever, headache, and fatigue, and in some cases can even be fatal. Early detection and treatment are absolutely vital. It's also important to take steps in preventing tick bites, such as using repellents and wearing appropriate clothing when in tick-infested areas. Stay safe out there, folks!
Elaine Curry
October 12, 2025 AT 20:35I couldn't help but notice you mentioned medication‑overuse headaches-gotta ask if you're on any pain meds daily? It's kind of weird how many people hide that from doctors maybe you should track it more closely.